

Last updated: 5/30/2015
Notice Of Employee Death {DIA 510}
Start Your Free Trial $ 13.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
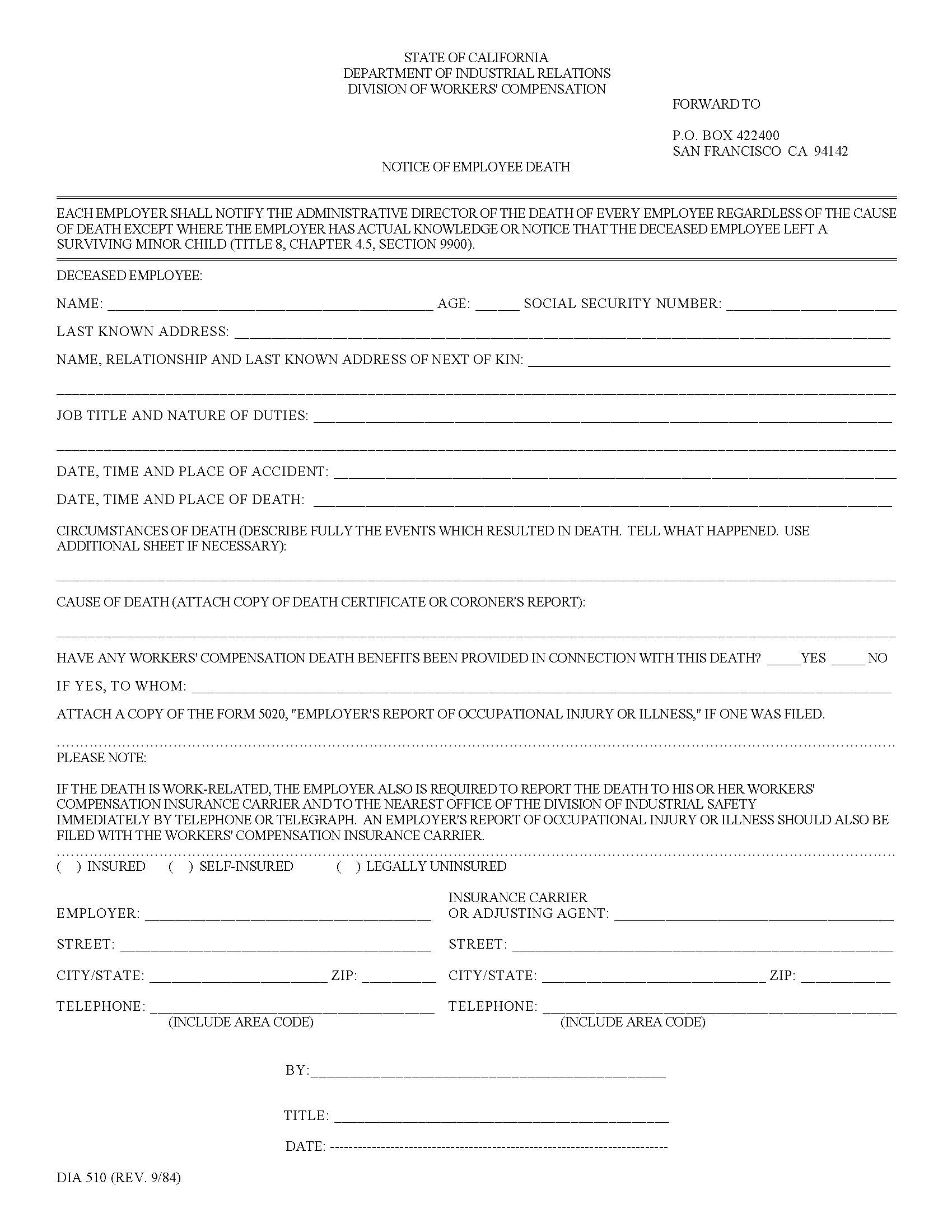
DIA 510 - NOTICE OF EMPLOYEE DEATH. This is a mandatory California Division of Workers’ Compensation reporting form that employers must submit to the Administrative Director whenever an employee dies, regardless of cause, unless the employer has actual knowledge that the deceased employee left a surviving minor child. The form collects essential information, including the employee’s identifying details, next of kin, job duties, circumstances of the accident and death, and cause of death, with a requirement to attach a death certificate or coroner’s report. Employers must also indicate whether death benefits have been provided and attach Form 5020 if previously filed. The form reminds employers of additional reporting duties to insurance carriers and Cal/OSHA for work-related fatalities. www.FormsWorkflow.com
Related forms
-

California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/Workers Comp/General/