

Last updated: 5/30/2015
DWC Medical Provider Network Complaint Form {DWC 9767.16.5}
Start Your Free Trial $ 13.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
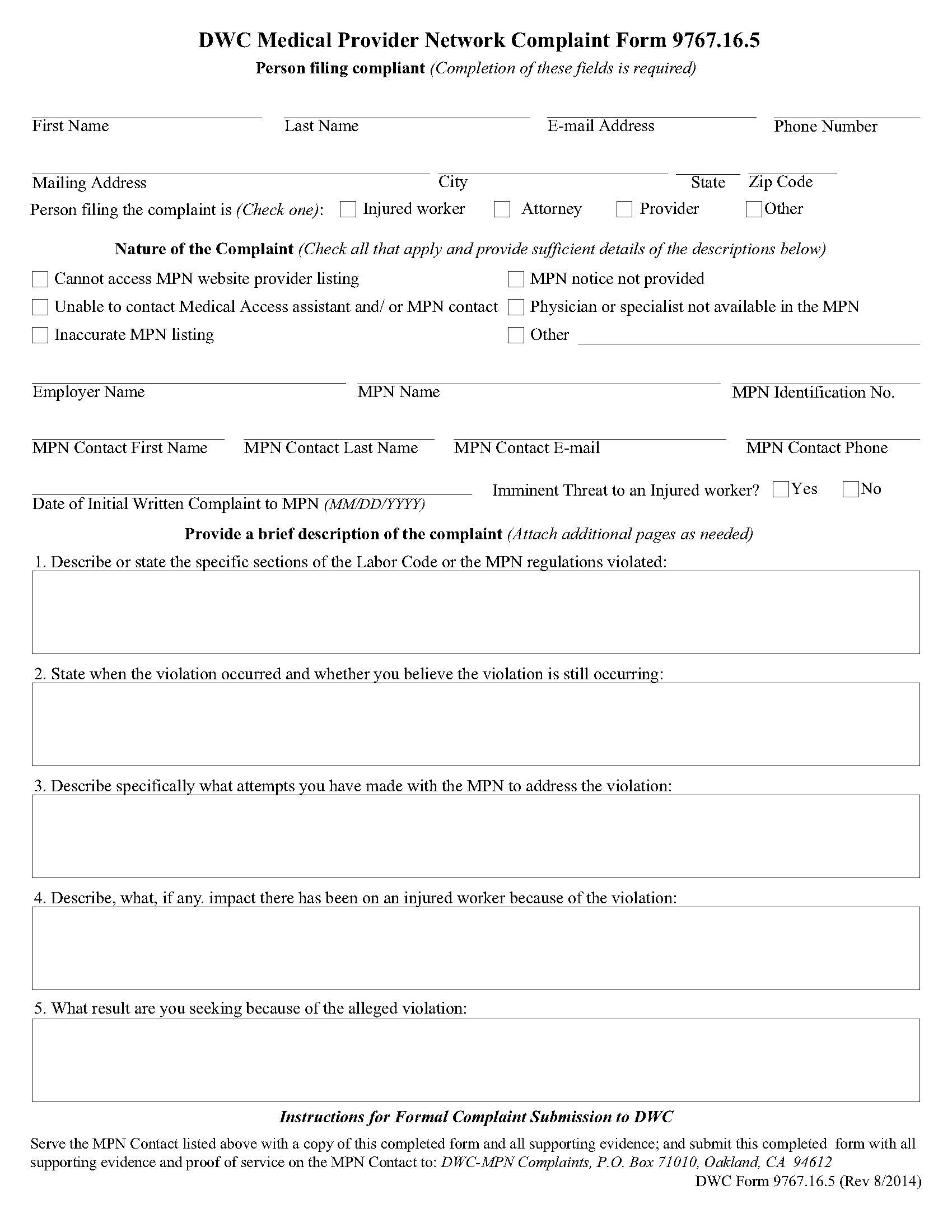
FORM 9767.16.5 - DWC MEDICAL PROVIDER NETWORK COMPLAINT. This is a California Division of Workers’ Compensation form used by injured workers, attorneys, medical providers, or other stakeholders to report violations of Medical Provider Network (MPN) requirements. The form allows complainants to document issues such as missing MPN notices, inaccessible medical access assistants, unavailable physicians or specialists, inaccurate provider listings, or problems accessing the MPN website. It collects key information about the complainant, employer, MPN, and MPN contact, and requires a detailed description of the alleged violation, including applicable Labor Code or regulatory sections, timelines, attempts to resolve the problem, and impact on the injured worker. Completed complaints must be served on the MPN contact and submitted to DWC with supporting evidence and proof of service. www.FormsWorkflow.com
Related forms
-

California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/Workers Comp/General/