

Last updated: 5/30/2015
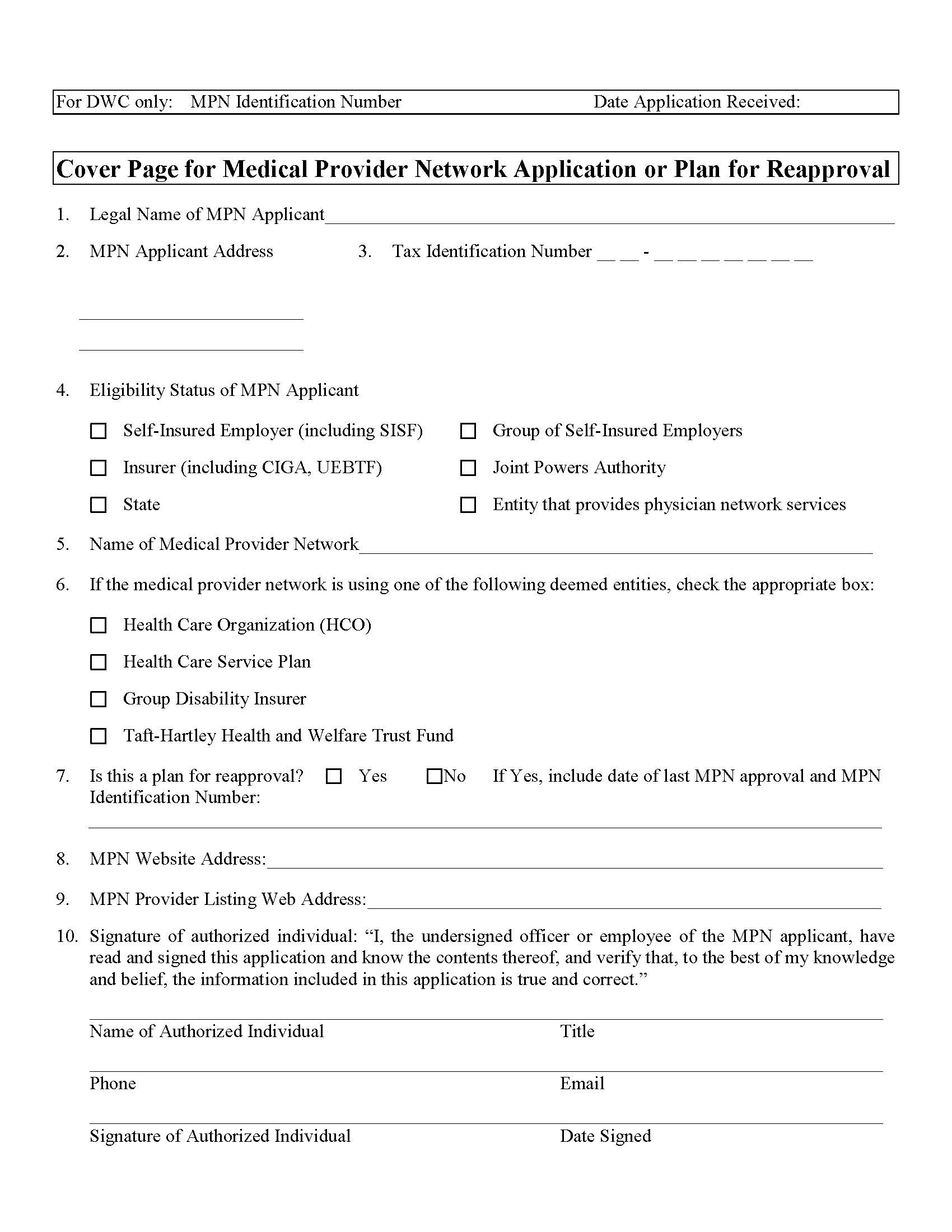
Cover Page For Medical Provider Network Application {DWC 9767.4}
Start Your Free Trial $ 13.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
COVER PAGE FOR MEDICAL PROVIDER NETWORK APPLICATION OR PLAN FOR REAPPROVAL. This is a mandatory California Division of Workers’ Compensation form used by insurers, self-insured employers, joint powers authorities, and other eligible entities to submit a new Medical Provider Network (MPN) application or request reapproval of an existing network. The form collects key administrative details, including the applicant’s legal name, address, tax ID, eligibility status, network name, deemed entity type (such as HCO or health care service plan), and website information. Applicants must also provide reapproval data when applicable and designate both an authorized signatory and an official liaison to the DWC. Completed forms must be submitted in duplicate along with the full MPN plan in searchable PDF format on digital media. www.FormsWorkflow.com
Related forms
-

California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/Workers Comp/General/ -
California/6 Workers Comp/General/ -
California/Workers Comp/General/