

Last updated: 5/2/2006
Medicare-Medicaid Psychiatirc Hospital Survey Data {CMS-724}
Start Your Free Trial $ 13.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
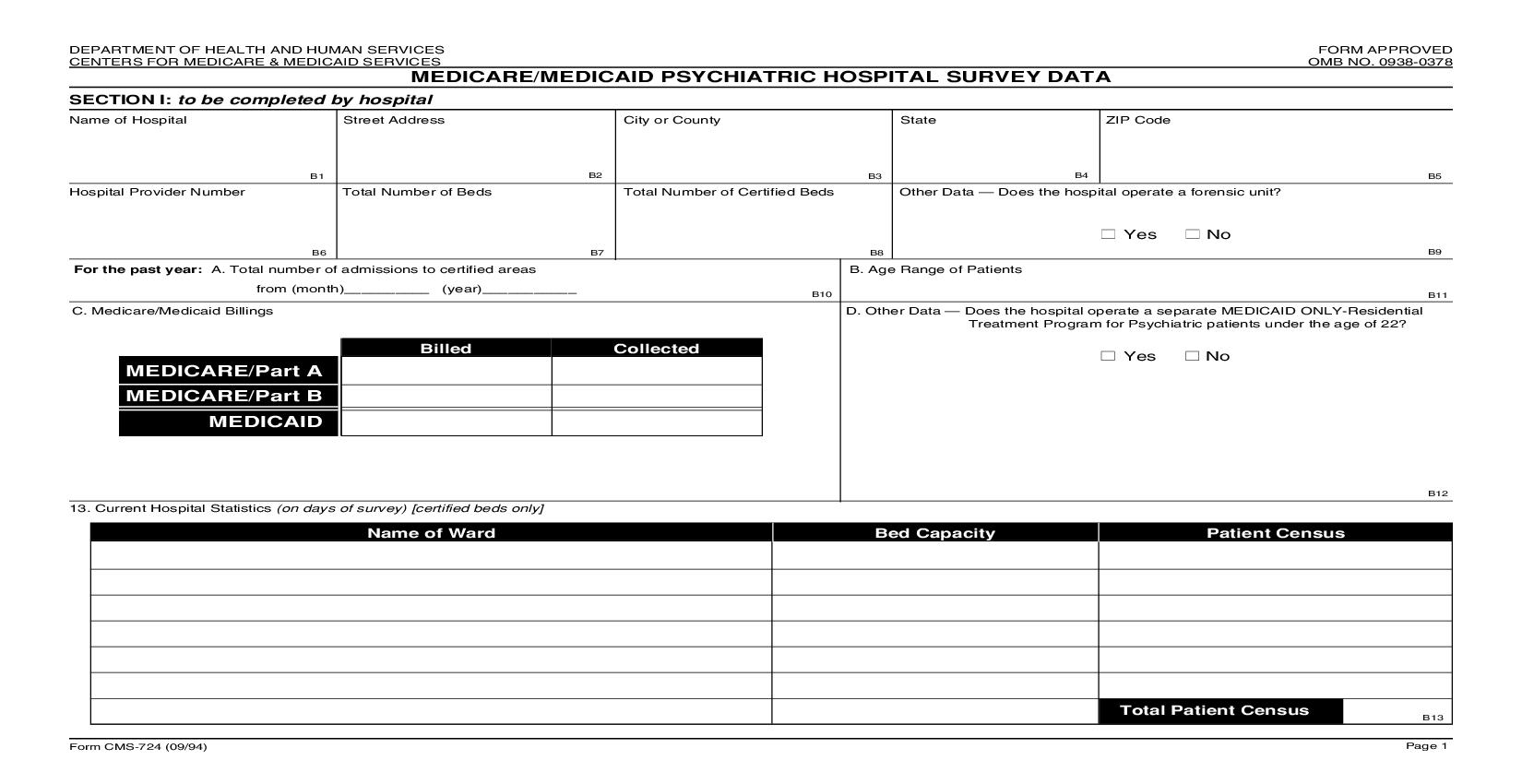
DEPARTMENT OF HEALTH AND HUMAN SERVICES FORM APPROVED CENTERS FOR MEDICARE & MEDICAID SERVICES OMB NO. 0938-0378 MEDICARE/MEDICAID PSYCHIATRIC HOSPITAL SURVEY DATA SECTION I: to be completed by hospital Name of Hospital Street Address City or County State ZIP Code B1 B2 B3 B4 B5 Hospital Provider Number Total Number of Beds Total Number of Certified Beds Other Data Does the hospital operate a forensic unit? Yes No B6 B7 B8 B9 For the past year: A. Total number of admissions to certified areas B. Age Range of Patients from (month)__________ (year)___________ B10 B11 C. Medicare/Medicaid Billings D. Other Data Does the hospital operate a separate MEDICAID ONLY-Re sidential Treatment Program for Psychiatric patients under the age of 22? Billed Collected Yes No MEDICARE/Part A MEDICARE/Part B MEDICAID B12 13. Current Hospital Statistics (on days of survey) [certified beds only] Name of Ward Bed Capacity Patient Census Total Patient Census B13 Form CMS-724 (09/94) Page 1<<<<<<<<<********>>>>>>>>>>>>> 2DEPARTMENT OF HEALTH AND HUMAN SERVICES FORM APPROVED CENTERS FOR MEDICARE & MEDICAID SERVICES OMB NO. 0938-0378 MEDICARE/MEDICAID PSYCHIATRIC HOSPITAL SURVEY DATA (contd) SECTION II: to be completed by the survey team Dates of Survey (beginning) Dates of Survey (ending date) Type of Survey: Initial (B16) Recertification (B17) Follow-up (B18) ___ ___/ ___ ___/ ___ ___ ___ ___/ ___ ___/ ___ ___ Complaint (B19) Second Follow-up (B20) Concurrent with (mm) (day) (year) (mm) (day) (year) General Hospital (B21) B14 B15 Survey Team Composition Total Number of Surveyors on Site Administrator (B22) SA (B32) Nurse (B23) RO (B33) Dietician (B24) Consultant (B34) Pharmacist (B25) CO (B35) Social Worker (B26) LSC Specialist (B27) Sanitarian (B28) Physician (B29) Psychologist (B30) Total Number of Surveyors on Site ________ (B36) Other ___________ (B31) 19. Certification of Findings I certify that I have reviewed each Condition of Participation and Relat ed Standards for Psychiatric Hospitals, and unless indicated on the CMS-2567, the Facility was found to be in compliance with the Conditions and/or St andards. Signature Title Date Signature Title Date Signature Title Date Signature Title Date According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is 0938-0378. The time required to complete this information collection is estimated to average 15 minutes per response, including the time to review instructions, search existing data resources, gather the data needed, and complete and review the information collection. If you have any comments concerning the accuracy of the time estimate(s) or suggestions for improving this form, please write to: CMS, Attn: PRA Reports Clearance Officer, 7500 Security Boulevard, Baltimore, Maryland 21244-1850. Form CMS-724 (09/94) Page 2
Related forms
-

Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/