

Last updated: 1/13/2020
Medicare Reconsideration Request Form {CMS-20033}
Start Your Free Trial $ 13.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
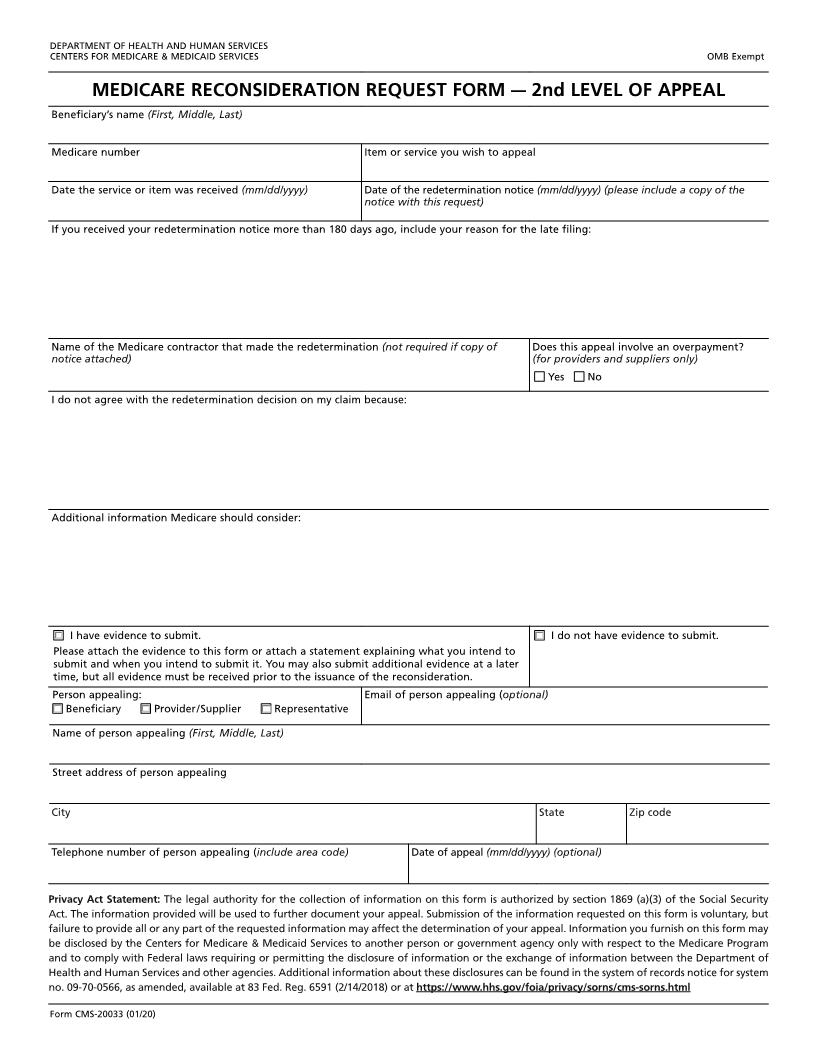
DEPARTMENTOF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE RECONSIDERATION REQUEST FORM 1. Beneficiarys Name:_____________________________________________________________________ 2. Medicare Number:______________________________________________________________________ 3. Description of Item or Service in Question:__________________________________________________ 4. Date the Service or Item was Received:_____________________________________________________ 5. I do not agree with the determination of my claim. MYREASONS ARE: ________________________________________________________________________ _____________ ________________________________________________________________________ _____________ ________________________________________________________________________ _____________ 6.Date of the redetermination notice__________________________________________________________ (If you received your redetermination more than 180 days ago, include your reason for not making this request earlier.) ________________________________________________________________________ _____________ ________________________________________________________________________ _____________ ________________________________________________________________________ _____________ 7. Additional Information Medicare Should Consider:____________________________________________ ________________________________________________________________________ _____________ ________________________________________________________________________ _____________ ________________________________________________________________________ _____________ 8. Requesters Name: ______________________________________________________________________ 9. Requesters Relationship to the Beneficiary: _________________________________________________ 10. Requesters Address: ____________________________________________________________________ ________________________________________________________________________ _____________ 11. Requesters T elephone Number:___________________________________________________________ 12. Requesters Signature: ___________________________________________________________________ 13. Date Signed:________________________________________________________________________ __ 14.o I have evidence to submit. (Attach such evidence to this form.) o I donot have evidence to submit. 15. Name of the Medicare Contractor that Made the Redetermination:________________________________ NOTICE: Anyone who misrepresents or falsifies essential information requested by this form may upon conviction be subject to fine or imprisonment under Federal Law. Form CMS -20033 (05/05) EF (045/2005) American LegalNet, Inc. www.USCourtForms.com
Related forms
-

Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/ -
Official Federal Forms/Centers For Medicare And Medicaid Services/