

Last updated: 11/18/2021
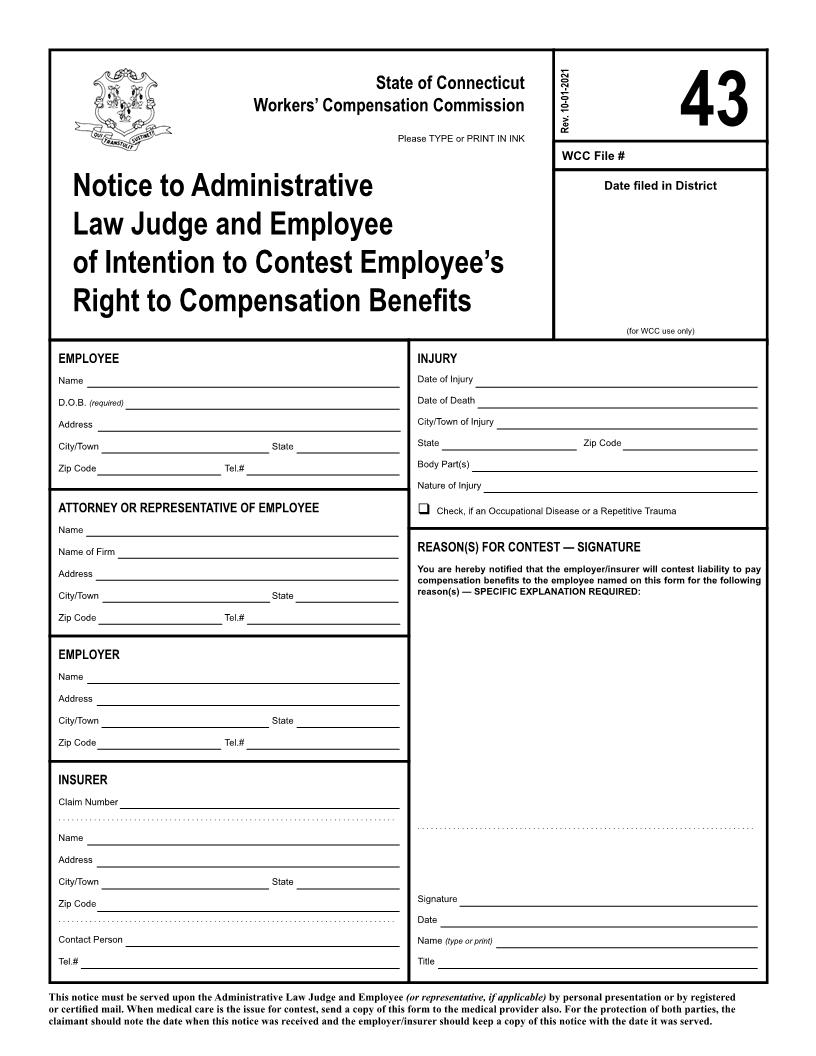
Notice To Compensation Commissioner And Employee Of Intention To Contest Employees Right To Compensation Benefits {43}
Start Your Free Trial $ 13.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
<document>COURT COUNTY OF43 Please TYPE or PRINT IN INK. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .:::::::Index No.2002 State of Connecticut Workers' Compensation Commission22-Calendar No.7-JUDICIAL SUBPOENAPlaintiff(s) -against-Defendant(s)WCC File # Rev.Date filed in DistrictNotice to Compensation Commissioner and Employee of Intention to Contest Employee's Right to Compensation Benefits. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .(for WCC use only)THE PEOPLE OF THE STATE OF NEW YORK TOInjury EmployeeNameSoc. Sec.# (optional) D.O.B. AddressCity/TownDate of Injury Date of Death City/Town of Injury StateZip CodeGREETINGS:StateBody Part(s) Nature of InjuryWE COMMAND YOU, that all business and excuses being laid aside, you and each of you attend before Court at the the HonorableZip CodeTel.#,located at County ofAttorney or Representative of Employee Check, if an Occupational Disease or a Repetitive Traumao'clock in the day of, on the, 20, at or adjourned date, to testify and give evidence as a witness in this action on the part of thenoon, and at any recessed in roomReason(s) for Contest Signature You are hereby notified that the employer/insurer will contest liability to pay compensation benefits to the employee named on this form for the following reason(s) SPECIFIC EXPLANATION REQUIRED:NameName of Firm AddressCity/TownStateYour failure to comply with this subpoena is punishable as a contempt of court and will make you liable to the party on whose behalf this subpoena was issued for a maximum penalty of $50 and all damages sustained as a result of your failure to comply.Zip CodeTel.#Employer, one of the Justices of theNameAddressCity/TownCourt in Witness, Honorableday of, 20 County,StateZip CodeTel.#(Attorney must sign above and type name below)InsurerClaim Number . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . NameAddressCity/TownAttorney(s) for. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .StateOffice and P.O. AddressSignatureDateName (typeorprint) TitleZip Code . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Contact Person Tel.#Telephone No.: Facsimile No.: E-Mail Address:This notice must be served upon the Commissioner and Employee (orrepresentative,ifapplicable)by personal presentation or by registered or certified mail. When medical care is the issue for contest, send a copy of this form to the medical provider also. For the protection of both parties, the claimant should note the date when this notice was received and the employer/insurer should keep a copy of this notice with the date it was served.Mobile Tel. No.:American LegalNet, Inc. www.USCourtForms.com</document>
Related forms
-

Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/