

Last updated: 11/18/2021
Hearing Cancellation Request {HC}
Start Your Free Trial $ 13.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
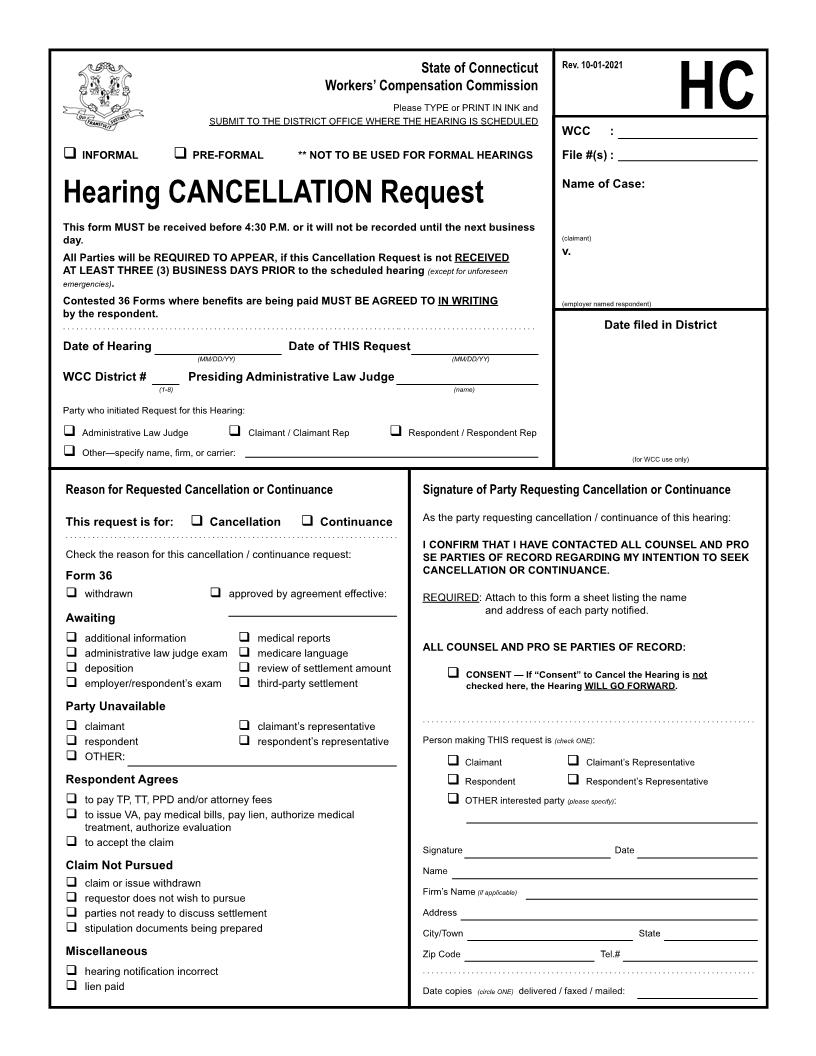
State of Connecticut Workers' Compensation Commission Please TYPE or PRINT IN INK and SUBMIT TO THE DISTRICT OFFICE WHERE THE HEARING IS SCHEDULED Rev. 12-22-2005 HC WCC : Hearing CANCELLATION Request I hereby request the Workers' Compensation Commission to CANCEL the following hearing: Informal Pre-Formal All Parties will be REQUIRED TO APPEAR, if this Cancellation Request is not RECEIVED AT LEAST THREE (3) BUSINESS DAYS PRIOR to the scheduled hearing (except for unforeseen emergencies). Contested 36 Forms where benefits are being paid MUST BE AGREED TO IN WRITING by the respondent. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . File #(s) : Name of Case: (claimant) v. Date filed in District Date of Hearing (MM/DD/YY) Date of THIS Request (MM/DD/YY) WCC District # (1-8) Presiding Commissioner (name) Party who initiated Request for this Hearing: Commissioner Claimant / Claimant Rep Respondent / Respondent Rep (for WCC use only) Other--specify name, firm, or carrier: Reason for Requested Cancellation or Continuance This request is for: Cancellation Continuance Signature of Party Requesting Cancellation or Continuance As the party requesting cancellation / continuance of this hearing: I CONFIRM THAT I HAVE CONTACTED ALL COUNSEL AND PRO SE PARTIES OF RECORD REGARDING MY INTENTION TO SEEK CANCELLATION OR CONTINUANCE. REQUIRED: Attach to this form a sheet listing the name and address of each party notified. All Counsel and Pro Se Parties of Record: Consent Do NOT Consent--explain here: ................................................................................... Check the reason for this cancellation / continuance request: Form 36 withdrawn approved by agreement effective: Awaiting additional information commissioner exam deposition IME medical reports medicare language review of settlement amount third-party settlement Party Unavailable claimant respondent OTHER: claimant's representative respondent's representative ................................................................................... Person making THIS request is Claimant Respondent (check ONE): Claimant's Representative Respondent's Representative (please specify): Respondent Agrees to pay TP, TT, PPD and/or attorney fees to issue VA, pay medical bills, pay lien, authorize medical treatment, authorized evaluation to accept the claim OTHER interested party Signature Name Firm's Name Address City/Town Zip Code (if applicable) Date Claim Not Pursued claim or issue withdrawn requestor does not wish to pursue parties not ready to discuss settlement stipulation documents being prepared State Tel.# Miscellaneous hearing notification incorrect lien paid ................................................................................... Date copies (circle ONE) delivered / faxed / mailed: American LegalNet, Inc. www.FormsWorkflow.com
Related forms
-

Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/