

Last updated: 7/11/2012
Employee Medical And Work Status Form
Start Your Free Trial $ 13.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
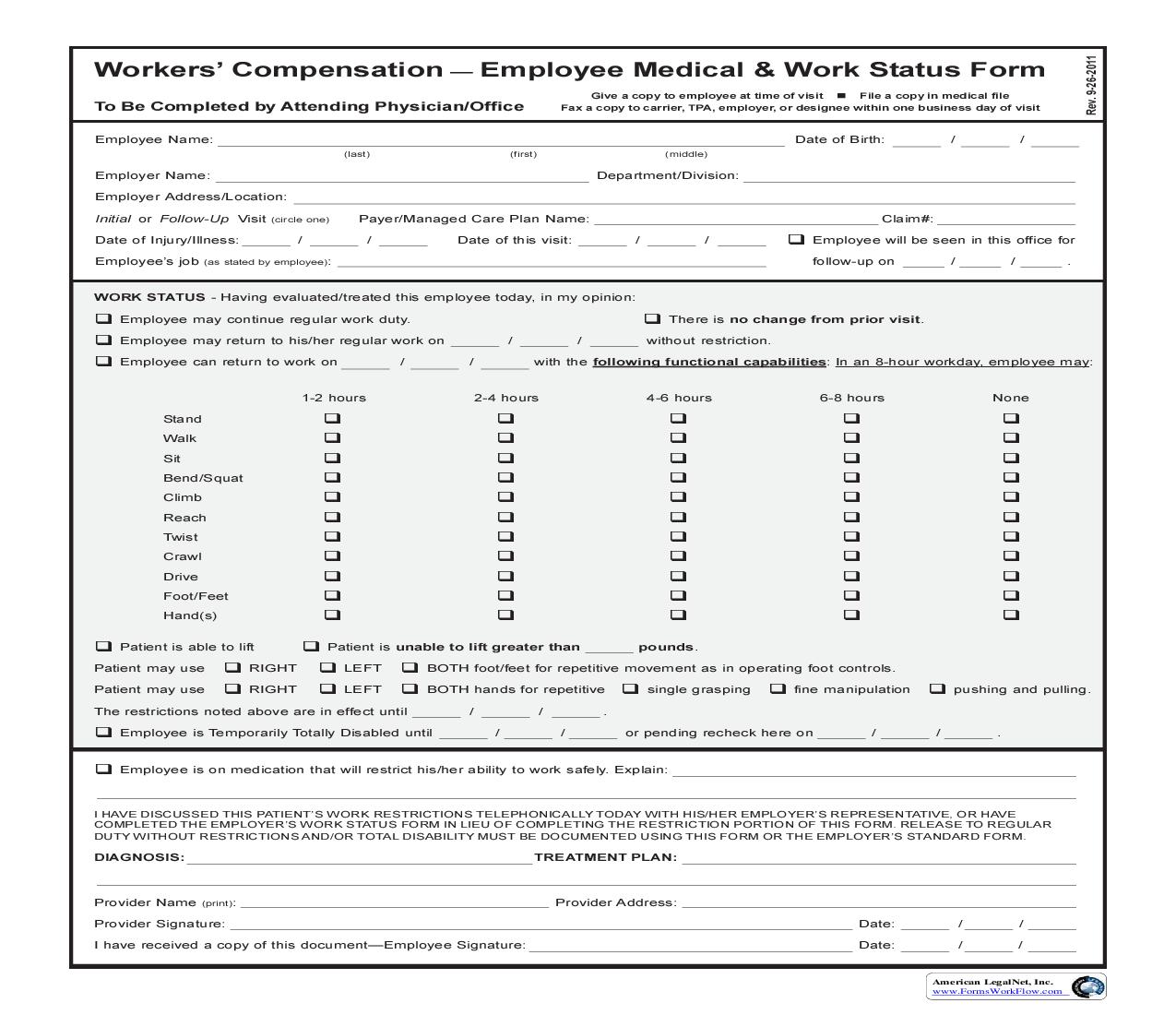
Workers Compensation Employee Medical & Work Status Form To Be Completed by Attending Physician/Office Employee Name: (last) (first) (middle) Give a copy to employee at time of visit n File a copy in medical file Fax a copy to carrier, TPA, employer, or designee within one business day of visit Date of Birth: Department/Division: / / Employer Name: Employer Address/Location: Initial or Follow-Up Visit Date of Injury/Illness: Employees job (circle one) Payer/Managed Care Plan Name: / Date of this visit: / / Claim#: / q Employee will be seen in this office for follow-up on / / . (as stated by employee): WORK STATUS - Having evaluated/treated this employee today, in my opinion: q q q Employee may continue regular work duty. Employee may return to his/her regular work on Employee can return to work on 1-2 hours Stand Walk Sit Bend/Squat Climb Reach Twist Crawl Drive Foot/Feet Hand(s) / / / / q There is no change from prior visit. without restriction. with the following functional capabilities: In an 8-hour workday, employee may: 2-4 hours 4-6 hours 6-8 hours None q q q q q q q q q q q q q q q q q q q q q q q q q q q q q q q q q q q q q q pounds. q q q q q q q q q q q q q q q q q q q q q q q Patient is able to lift Patient is unable to lift greater than LEFT LEFT Patient may use Patient may use q q RIGHT RIGHT BOTH foot/feet for repetitive movement as in operating foot controls. BOTH hands for repetitive / / / / . or pending recheck here on / / . q single grasping q fine manipulation q pushing and pulling. The restrictions noted above are in effect until q q Employee is Temporarily Totally Disabled until Employee is on medication that will restrict his/her ability to work safely. Explain: I HAVE DISCUSSED THIS PATIENTS WORK RESTRICTIONS TELEPHONICALLY TODAY WITH HIS/HER EMPLOYERS REPRESENTATIVE, OR HAVE COMPLETED THE EMPLOYERS WORK STATUS FORM IN LIEU OF COMPLETING THE RESTRICTION PORTION OF THIS FORM. RELEASE TO REGULAR DUTY WITHOUT RESTRICTIONS AND/OR TOTAL DISABILITY MUST BE DOCUMENTED USING THIS FORM OR THE EMPLOYERS STANDARD FORM. DIAGNOSIS: TREATMENT PLAN: Provider Name (print): Provider Address: Date: Date: / / / / Provider Signature: I have received a copy of this documentEmployee Signature: American LegalNet, Inc. www.FormsWorkFlow.com Rev. 9-26-2011
Related forms
-

Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/ -
Connecticut/Workers Compensation/