

Last updated: 4/13/2015
Workers Compensation Insurance Affidavit - General Businesses
Start Your Free Trial $ 13.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
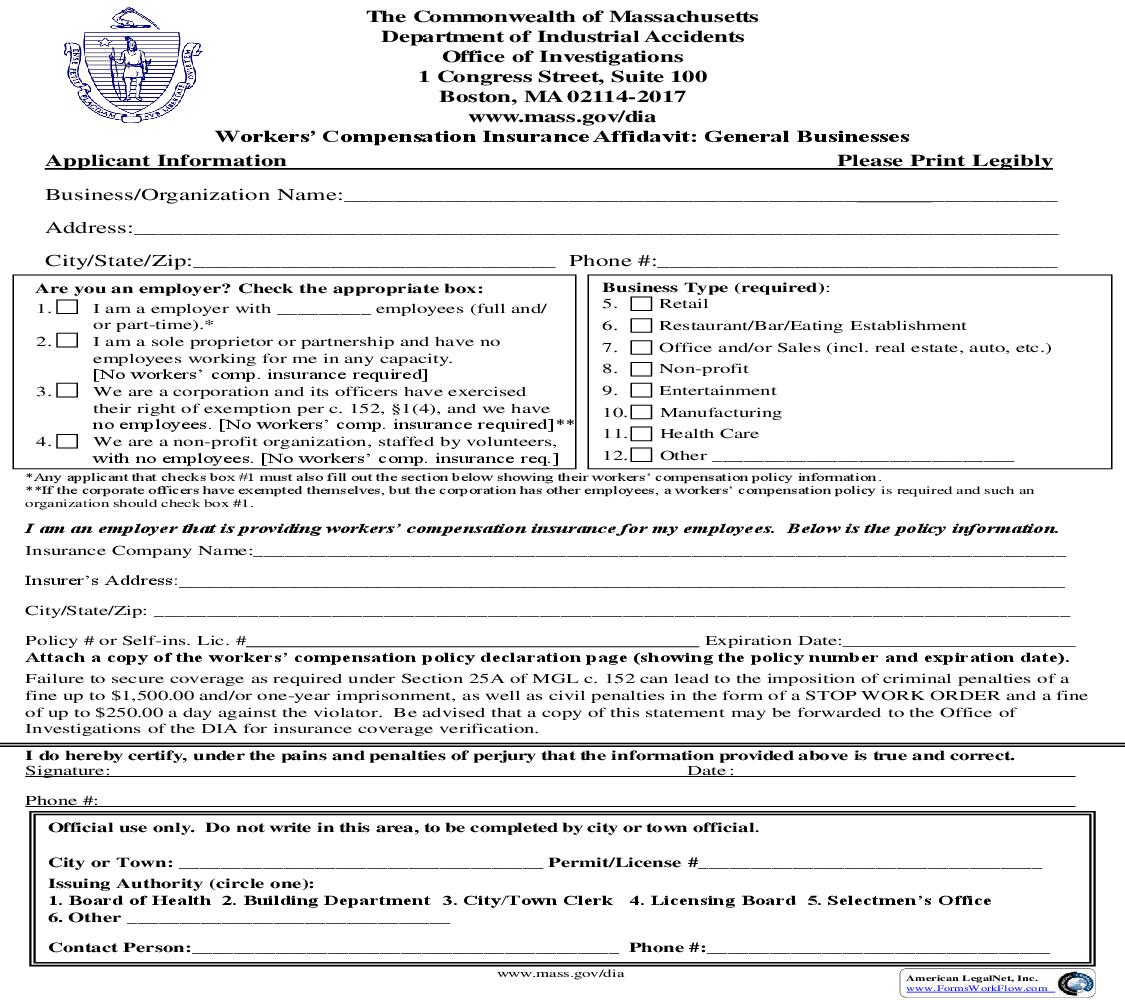
The Commonwealth of Massachusetts Department of Industrial Accidents Office of Investigations 1 Congress Street, Suite 100 Boston, MA 02114-2017 www.mass.gov/dia Workers' Compensation Insurance Affidavit: General Businesses Applicant Information Please Print Legibly Business/Organization Name:_________________________________________ __________ Address:__________________________________________________________________________ City/State/Zip:_____________________________ Phone #:________________________________ Are you an employer? Check the appropriate box: 1. I am a employer with _________ employees (full and/ or part-time).* 2. I am a sole proprietor or partnership and have no employees working for me in any capacity. [No workers' comp. insurance required] 3. We are a corporation and its officers have exercised their right of exemption per c. 152, §1(4), and we have no employees. [No workers' comp. insurance required]** 4. We are a non-profit organization, staffed by volunteers, with no employees. [No workers' comp. insurance req.] Business Type (required): 5. Retail 6. 7. 8. 9. 10. 11. 12. Restaurant/Bar/Eating Establishment Office and/or Sales (incl. real estate, auto, etc.) Non-profit Entertainment Manufacturing Health Care Other _____________________________ *Any applicant that checks box #1 must also fill out the section below showing their workers' compensation policy information. **If the corporate officers have exempted themselves, but the corporation has other employees, a workers' compensation policy is required and such an organization should check box #1. I am an employer that is providing workers' compensation insurance for my employees. Below is the policy information. Insurance Company Name:______________________________________________________________________________ Insurer's Address:_____________________________________________________________________________________ City/State/Zip: ________________________________________________________________________________________ Policy # or Self-ins. Lic. # Expiration Date: Attach a copy of the workers' compensation policy declaration page (showing the policy number and expiration date). Failure to secure coverage as required under Section 25A of MGL c. 152 can lead to the imposition of criminal penalties of a fine up to $1,500.00 and/or one-year imprisonment, as well as civil penalties in the form of a STOP WORK ORDER and a fine of up to $250.00 a day against the violator. Be advised that a copy of this statement may be forwarded to the Office of Investigations of the DIA for insurance coverage verification. I do hereby certify, under the pains and penalties of perjury that the information provided above is true and correct. Signature: Date : Phone #: Official use only. Do not write in this area, to be completed by city or town official. City or Town: ___________________________________ Permit/License #_________________________________ Issuing Authority (circle one): 1. Board of Health 2. Building Department 3. City/Town Clerk 4. Licensing Board 5. Selectmen's Office 6. Other _______________________________ Contact Person:_________________________________________ Phone #:_________________________________ www.mass.gov/dia American LegalNet, Inc. www.FormsWorkFlow.com Information and Instructions Massachusetts General Laws chapter 152 requires all employers to provide workers' compensation for their employees. Pursuant to this statute, an employee is defined as "...every person in the service of another under any contract of hire, express or implied, oral or written." An employer is defined as "an individual, partnership, association, corporation or other legal entity, or any two or more of the foregoing engaged in a joint enterprise, and including the legal representatives of a deceased employer, or the receiver or trustee of an individual, partnership, association or other legal entity, employing employees. However, the owner of a dwelling house having not more than three apartments and who resides therein, or the occupant of the dwelling house of another who employs persons to do maintenance, construction or repair work on such dwelling house or on the grounds or building appurtenant thereto shall not because of such employment be deemed to be an employer." MGL chapter 152, §25C(6) also states that "every state or local licensing agency shall withhold the issuance or renewal of a license or permit to operate a business or to construct buildings in the commonwealth for any applicant who has not produced acceptable evidence of compliance with the insurance coverage required." Additionally, MGL chapter 152, §25C(7) states "Neither the commonwealth nor any of its political subdivisions shall enter into any contract for the performance of public work until acceptable evidence of compliance with the insurance requirements of this chapter have been presented to the contracting authority." Applicants Please fill out the workers' compensation affidavit completely, by checking the boxes that apply to your situation and, if necessary, supply your insurance company's name, address and phone number along with a certificate of insurance. Limited Liability Companies (LLC) or Limited Liability Partnerships (LLP) with no employees other than the members or partners, are not required to carry workers' compensation insurance. If an LLC or LLP does have employees, a policy is required. Be advised that this affidavit may be submitted to the Department of Industrial Accidents for confirmation of insurance coverage. Also be sure to sign and date the affidavit. The affidavit should be returned to the city or town that the application for the permit or license is being requested, not the Department of Industrial Accidents. Should you have any questions regarding the law or if you are required to obtain a workers' compensation policy, please call the Department at the number listed below. Self-insured companies should enter their self-insurance license number on the appropriate line. City or Town Officials Please be sure that the affidavit is complete and printed legibly. The Department has provided a space at the bottom of the affidavit for you to fill out in the event the Office of Investigations has to contact you regarding the applicant. Please be sure to fill in the permit/license number which will be used as a reference number. In addition, an applicant that must submit multiple permit/license applications in any given year, need onl
Related forms
-

Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/6 Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/6 Workers Comp/ -
Massachusetts/6 Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/6 Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/