

Last updated: 4/17/2017
Agreement To Extend 180 Day Payment Without Prejudice Period {105}
Start Your Free Trial $ 13.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
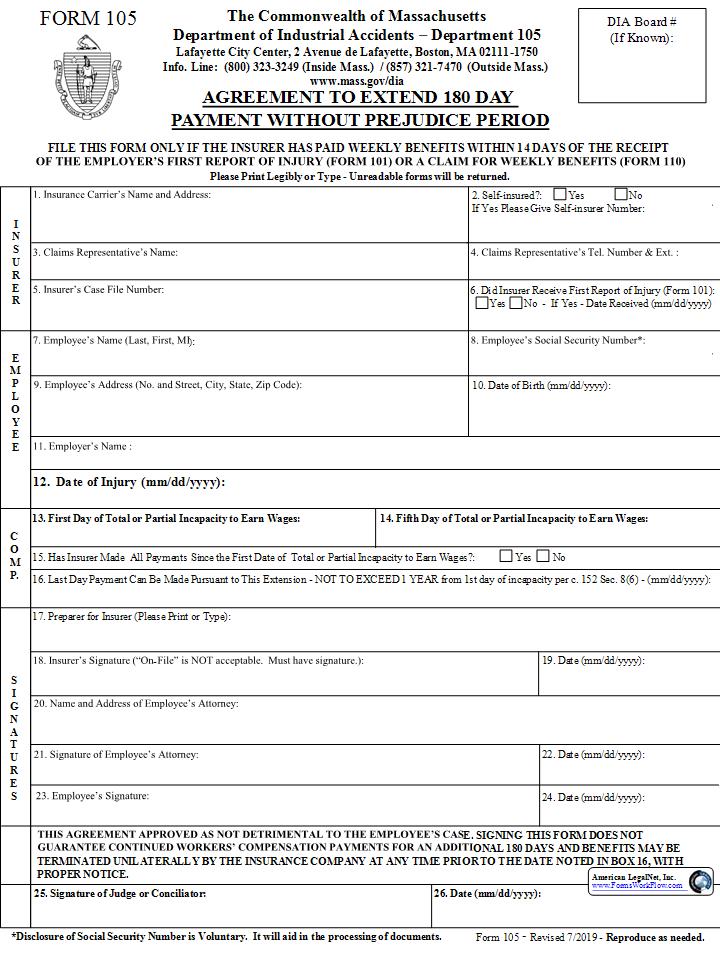
FORM 105 1 Congress Street, Suite 100, Boston, Massachusetts 02114-2017 Info. Line 800-323-3249 ext. 7470 in Mass. Outside Mass. - 617-727-4900 ext. 7470 http://www.mass.gov/dia The Commonwealth of Massachusetts Department of Industrial Accidents Department 105 DIA Board # (If Known): AGREEMENT TO EXTEND 180 DAY PAYMENT WITHOUT PREJUDICE PERIOD Please Print Legibly or Type - Unreadable forms will be returned. FILE THIS FORM ONLY IF THE INSURER HAS PAID WEEKLY BENEFITS WITHIN 14 DAYS OF THE RECEIPT OF THE EMPLOYER'S FIRST REPORT OF INJURY (FORM 101) OR A CLAIM FOR WEEKLY BENEFITS (FORM 110) 1. Insurance Carrier's Name and Address: I N S U R E R 2. Self-insured?: Yes No If Yes Please Give Self-insurer Number: 3. Claims Representative's Name: 5. Insurer's Case File Number: 4. Claims Representative's Tel. Number & Ext. : 6. Did Insurer Receive First Report of Injury (Form 101): Yes No - If Yes - Date Received (mm/dd/yyyy) 8. Employee's Social Security Number*: 7. Employee's Name (Last, First, MI): E M P L O Y E E 9. Employee's Address (No. and Street, City, State, Zip Code): 10. Date of Birth (mm/dd/yyyy): 11. Employer's Name : 12. Date of Injury (mm/dd/yyyy): 13. First Day of Total or Partial Incapacity to Earn Wages: C O M P. 14. Fifth Day of Total or Partial Incapacity to Earn Wages: Yes No 15. Has Insurer Made All Payments Since the First Date of Total or Partial Incapacity to Earn Wages?: 16. Last Day Payment Can Be Made Pursuant to This Extension - NOT TO EXCEED 1 YEAR from 1st day of incapacity per c. 152 Sec. 8(6) - (mm/dd/yyyy): 17. Preparer for Insurer (Please Print or Type): 18. Insurer's Signature ("On-File" is NOT acceptable. Must have signature.): S I G N A T U R E S 19. Date (mm/dd/yyyy): 20. Name and Address of Employee's Attorney: 21. Signature of Employee's Attorney: 22. Date (mm/dd/yyyy): 23. Employee's Signature: 24. Date (mm/dd/yyyy): THIS AGREEMENT APPROVED AS NOT DETRIMENTAL TO THE EMPLOYEE'S CASE. SIGNING THIS FORM DOES NOT GUARANTEE CONTINUED WORKERS' COMPENSATION PAYMENTS FOR AN ADDITIONAL 180 DAYS AND BENEFITS MAY BE TERMINATED UNILATERALLY BY THE INSURANCE COMPANY AT ANY TIME PRIOR TO THE DATE NOTED IN BOX 16, WITH PROPER NOTICE. 25. Signature of Judge or Conciliator: 26. Date (mm/dd/yyyy): Form 105 - Revised 2/2017 - Reproduce as needed. American LegalNet, Inc. www.FormsWorkFlow.com *Disclosure of Social Security Number is Voluntary. It will aid in the processing of documents.
Related forms
-

Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/6 Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/6 Workers Comp/ -
Massachusetts/6 Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/6 Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/ -
Massachusetts/Workers Comp/