

Last updated: 4/17/2007
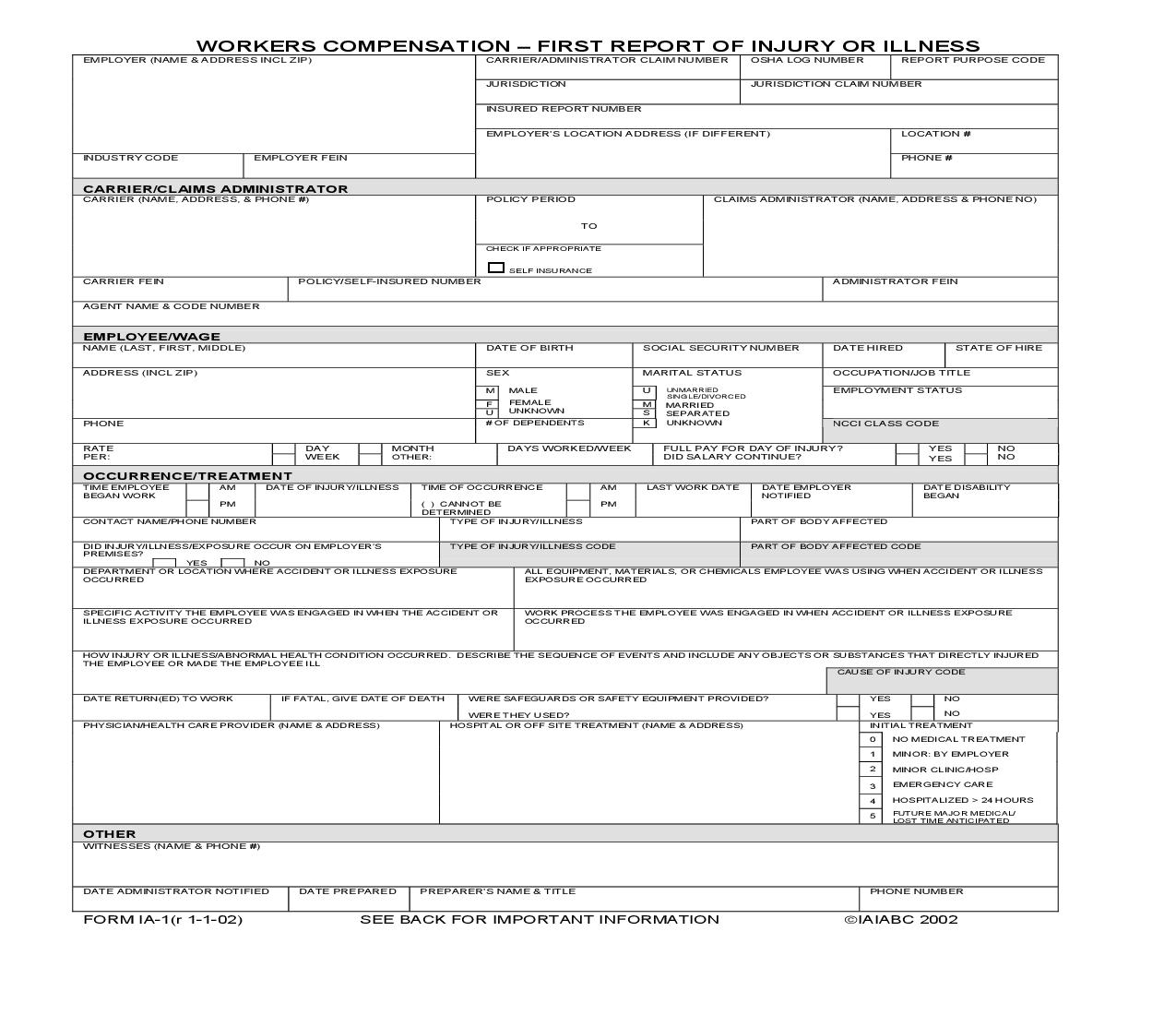
First Report Of Injury Or Illness {IA-1}
Start Your Free Trial $ 15.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
<document>COURT COUNTY OF. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .:::::::Index No.WORKERS COMPENSATION FIRST REPORT OF INJURY OR ILLNESS CARRIER/ADMINISTRATOR CLAIM NUMBER OSHA LOG NUMBERREPORT PURPOSE CODECalendar No.JURISDICTIONJURISDICTION CLAIM NUMBERINSURED REPORT NUMBER EMPLOYER (NAME & ADDRESS INCL ZIP)JUDICIAL SUBPOENAPlaintiff(s)LOCATION #EMPLOYER'S LOCATION ADDRESS (IF DIFFERENT)-against-INDUSTRY CODEEMPLOYER FEINPHONE #CARRIER/CLAIMS ADMINISTRATOR CARRIER (NAME, ADDRESS, & PHONE #)CLAIMS ADMINISTRATOR (NAME, ADDRESS & PHONE NO) POLICY PERIODTODefendant(s). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .CHECK IF APPROPRIATE SELF INSURANCECARRIER FEINPOLICY/SELF-INSURED NUMBERADMINISTRATOR FEINTHE PEOPLE OF THE STATE OF NEW YORK TOAGENT NAME & CODE NUMBEREMPLOYEE/WAGE NAME (LAST, FIRST, MIDDLE)DATE OF BIRTHSOCIAL SECURITY NUMBERDATE HIREDSTATE OF HIRESEXMARITAL STATUSOCCUPATION/JOB TITLEMALEFEMALEUNKNOWNMUUNMARRIEDSINGLE/DIVORCEDEMPLOYMENT STATUSGREETINGS:FM ADDRESS (INCL ZIP)MARRIEDSEPARATED K PHONESUUNKNOWN# OF DEPENDENTSNCCI CLASS CODEWE COMMAND YOU, that all business and excuses being laid aside, you and each of you attend before Court at the the HonorableMONTHOTHER:DAYWEEKNONODAYS WORKED/WEEKFULL PAY FOR DAY OF INJURY? DID SALARY CONTINUE?YES RATEPER:,YESlocated at County ofOCCURRENCE/TREATMENT TIME EMPLOYEE BEGAN WORKo'clock in the day of, on the, 20, at or adjourned date, to testify and give evidence as a witness in this action on the part of thenoon, and at any recessed in roomAMPMDATE OF INJURY/ILLNESSTIME OF OCCURRENCE ( ) CANNOT BE DETERMINEDAMPMLAST WORK DATEDATE EMPLOYER NOTIFIEDDATE DISABILITY BEGANCONTACT NAME/PHONE NUMBERTYPE OF INJURY/ILLNESSPART OF BODY AFFECTEDDID INJURY/ILLNESS/EXPOSURE OCCUR ON EMPLOYER'S PREMISES?TYPE OF INJURY/ILLNESS CODEPART OF BODY AFFECTED CODEYESNO DEPARTMENT OR LOCATION WHERE ACCIDENT OR ILLNESS EXPOSURE OCCURREDYour failure to comply with this subpoena is punishable as a contempt of court and will make you liable to the party on whose behalf this subpoena was issued for a maximum penalty of $50 and all damages sustained as a result of your failure to comply.ALL EQUIPMENT, MATERIALS, OR CHEMICALS EMPLOYEE WAS USING WHEN ACCIDENT OR ILLNESS EXPOSURE OCCURREDSPECIFIC ACTIVITY THE EMPLOYEE WAS ENGAGED IN WHEN THE ACCIDENT OR ILLNESS EXPOSURE OCCURREDWORK PROCESS THE EMPLOYEE WAS ENGAGED IN WHEN ACCIDENT OR ILLNESS EXPOSURE OCCURRED, one of the Justices of theCourt in Witness, Honorableday of, 20 County,HOW INJURY OR ILLNESS/ABNORMAL HEALTH CONDITION OCCURRED. DESCRIBE THE SEQUENCE OF EVENTS AND INCLUDE ANY OBJECTS OR SUBSTANCES THAT DIRECTLY INJURED THE EMPLOYEE OR MADE THE EMPLOYEE ILLCAUSE OF INJURY CODEIF FATAL, GIVE DATE OF DEATHYESYESNO DATE RETURN(ED) TO WORK(Attorney must sign above and type name below)NOWERE SAFEGUARDS OR SAFETY EQUIPMENT PROVIDED? WERE THEY USED?PHYSICIAN/HEALTH CARE PROVIDER (NAME & ADDRESS)HOSPITAL OR OFF SITE TREATMENT (NAME & ADDRESS)INITIAL TREATMENT 01234NO MEDICAL TREATMENT MINOR: BY EMPLOYER MINOR CLINIC/HOSP EMERGENCY CARE HOSPITALIZED > 24 HOURS FUTURE MAJOR MEDICAL/ LOST TIME ANTICIPATEDAttorney(s) for5OTHERWITNESSES (NAME & PHONE #)Office and P.O. AddressDATE ADMINISTRATOR NOTIFIEDPHONE NUMBERPREPARER'S NAME & TITLEDATE PREPAREDTelephone No.: Facsimile No.: E-Mail Address:FORM IA-1(r 1-1-02)2002SEE BACK FOR IMPORTANT INFORMATION. IAIABCMobile Tel. No.:American LegalNet, Inc. www.USCourtForms.comCOURT COUNTY OF. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .:::::::Index No.Calendar No.JUDICIAL SUBPOENAPlaintiff(s) -against-Defendant(s)EMPLOYER'S INSTRUCTIONS DO NOT ENTER DATA IN SHADED FIELDS. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .THE PEOPLE OF THE STATE OF NEW YORK TOGREETINGS:WE COMMAND YOU, that all business and excuses being laid aside, you and each of you attend before Court at the the Honorable,DATES: Enter all dates in MM/DD/YY format. INDUSTRY CODE: This is the code which represents the nature of the employer's business, which is contained in the Standard Industrial Classification Manual or the North American Industry Classification System, published by the Federal Office of Management and Budget. CARRIER:The licensed business entity issuing a contract of insurance and assuming financial responsibility on behalf of the employer of the claimant. CLAIMS ADMINISTRATOR: Enter the name of the carrier, third party administrator, state fund, or self-insured responsible for administering the claim. AGENT NAME & CODE NUMBER: Enter the name of your insurance agent and his/her code number if known. This information can be found on your insurance policy. OCCUPATION/JOB TITLE: This is the primary occupation of the claimant at the time of the accident or exposure. EMPLOYMENT STATUS: Indicate the employee's work status. The valid choices are: Full-Timelocated at County ofo'clock in the day of, on the, 20, at or adjourned date, to testify and give evidence as a witness in this action on the part of thenoon, and at any recessed in roomOn StrikeUnknownVolunteer Part-TimeDisabledApprenticeship Full-TimeSeasonal Not EmployedRetiredApprenticeship Part-TimePiece WorkerYour failure to comply with this subpoena is punishable as a contempt of court and will make you liable to the party on whose behalf this subpoena was issued for a maximum penalty of $50 and all damages sustained as a result of your failure to comply.DATE DISABILITY BEGAN: The first day on which the claimant originally lost time from work due to the occupation injury or disease or as otherwise designated by statute. CONTACT NAME/PHONE NUMBER: Enter the name of the individual at the employer's premises to be contacted for additional information. TYPE OF INJURY/ILLNESS: Briefly describe the nature of the injury or illness, (eg. Lacerations to the forearm). PART OF BODY AFFECTED: Indicate the part of body affected by the injury/illness, (eg. Right forearm, lower back). DEPARTMENT OR LOCATION WHERE ACCIDENT OR ILLNESS EXPOSURE OCCURRED: (eg. Maintenance Department or Client's office at 452 Monroe St., Washington, DC 26210), one of the Justices of theCourt in Witness, Honorableday of, 20 County,(Attorney must sign above and type name below)Attorney(s) forIf t
