

Last updated: 3/10/2025
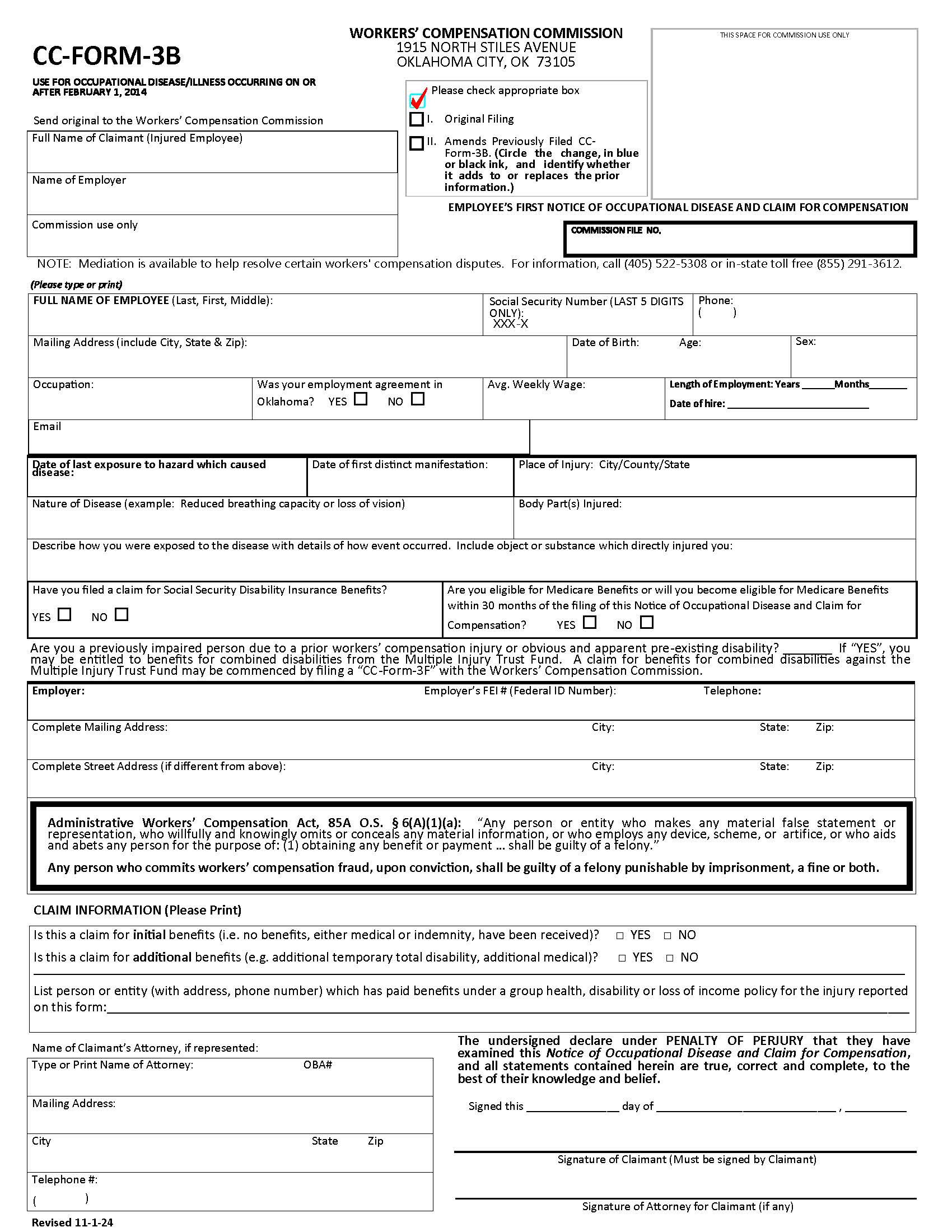
Employees First Notice Of Occupational Disease And Claim For Compensation {CC-Form-3B}
Start Your Free Trial $ 13.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
CC-FORM-3B - EMPLOYEE’S FIRST NOTICE OF OCCUPATIONAL DISEASE AND CLAIM FOR COMPENSATION. This form is used by employees to file with the Oklahoma Workers’ Compensation Commission for illnesses or diseases caused by workplace exposure. This form applies to occupational diseases or illnesses occurring on or after February 1, 2014 and serves as an official request for workers’ compensation benefits. The form requires the employee to provide details such as their personal information, employment history, date of last exposure to the hazardous condition, and the nature of the illness or disease. It also asks for a description of how the exposure occurred, any affected body parts, and whether the employee has filed for Social Security Disability or Medicare benefits. Additionally, the form collects information about the employer and any other entities that may have paid benefits related to the illness. www.FormsWorkflow.com
Related forms
-

Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/