

Last updated: 9/1/2023
Motion To Set For Trial {9}
Start Your Free Trial $ 13.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
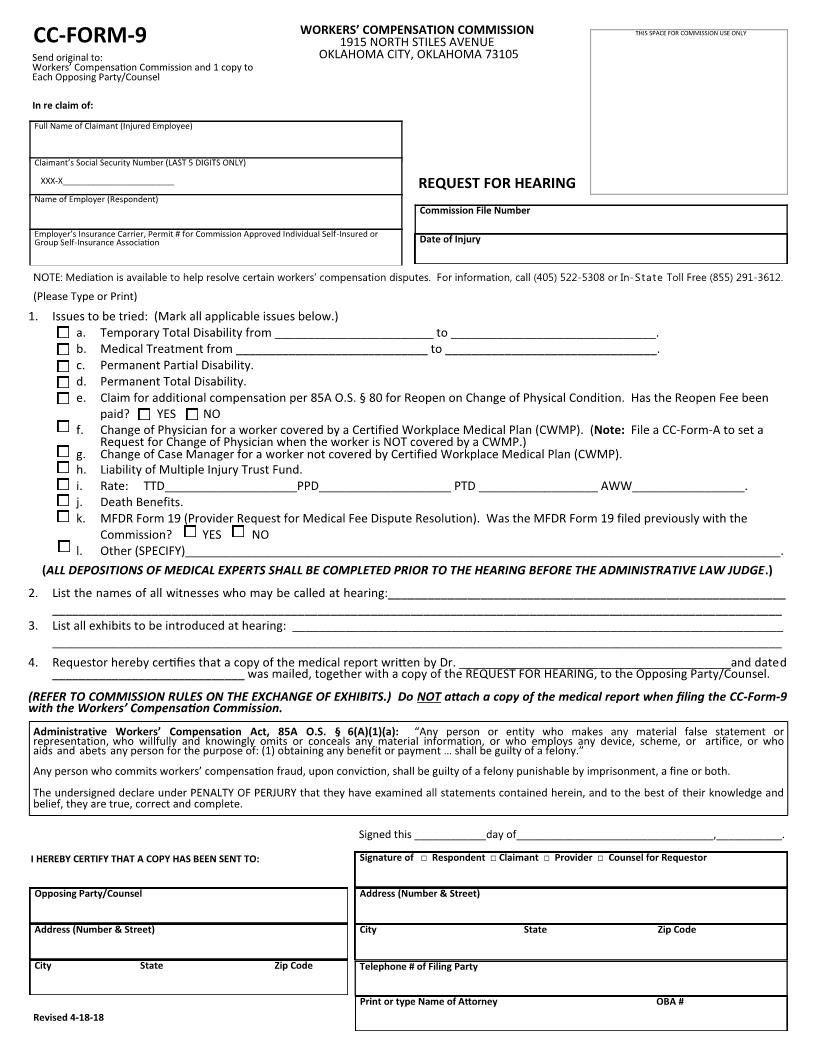
Send original to Court of Existing Claims and 1 copy to Each Opposing Party/Counsel In re claim of: Full Name of Claimant (Injured Employee) FORM 9 COURT OF EXISTING CLAIMS 1915 NORTH STILES, STE 127 OKLAHOMA CITY, OKLAHOMA 73105-4918 THIS SPACE FOR COURT USE ONLY Claimant's Social Security Number (LAST 4 DIGITS ONLY) XXX-XX-________________________ Name of Employer (Respondent) MOTION TO SET FOR TRIAL WCC FILE NO. Date of Injury Employer's Insurance Carrier, Permit # for Court Approved Individual Self-Insured or Group Self-Insurance Association NOTE: Mediation is available to address certain workers' compensation disputes. For information, call (918) 581-2714. (Please Type or Print) 1. Issues to be tried: (Circle all applicable issues below.) a. b. c. d. e. f. g. h. i. j. k. l. Temporary Total Disability from ________________________ to _______________________________. Medical Treatment from _____________________________ to ________________________________. Permanent Partial Disability/Permanent Partial Impairment. Permanent Total Disability. Motion to Reopen on Change of Condition. Has the Reopen Fee been paid? YES NO Change of Physician for a worker covered by a Certified Workplace Medical Plan (CWMP). (Note: File a Form A to set a request for Change of Physician when there is no CWMP.) Change of Case Manager for a worker not covered by Certified Workplace Medical Plan (CWMP). Liability of Multiple Injury Trust Fund. Rate: TTD____________________PPD/PPI____________________AWW_________________. Death Benefits. Appeal from Form 18 Order. Form 19 (Request For Payment of Health or Rehabilitation Services). Was the Form 19 filed previously? (ALL DEPOSITIONS OF MEDICAL EXPERTS SHALL BE COMPLETED PRIOR TO TRIAL.) 2. 3. 4. List the names of all witnesses who may be called at trial:________________________________________________________________ ______________________________________________________________________________________________________________ List all exhibits to be introduced at trial: ______________________________________________________________________________ ______________________________________________________________________________________________________________ Requestor hereby certifies that a copy of the medical report written by Dr. _______________________and dated ________________ was mailed, together with this motion, to Opposing Party/Counsel. (Refer to Court rules regarding the exchange of exhibits.) Do NOT attach a copy of the medical report when filing the Form 9 with the Court of Existing Claims. YES NO m. Other (SPECIFY)_____________________________________________________________________________________. I declare under penalty of perjury that I have examined this motion and all statements contained herein, and to the best of my knowledge and belief, they are true, correct and complete. Any person who commits workers' compensation fraud, upon conviction, shall be guilty of a felony. I HEREBY CERTIFY THAT A COPY HAS BEEN SENT TO: Opposing Party/Counsel Address (Number & Street) City State Zip Code Signed this____________day of__________________________,___________. Signature of Requesting Party Address (Number & Street) City State Zip Code claimant resp. med/rehab provider Telephone # of Requesting Party Print or type name of Attorney Rev. 06/24/2015 American LegalNet, Inc. www.FormsWorkFlow.com OBA #
Related forms
-

Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/ -
Oklahoma/Workers Comp/