Ohio
Statewide
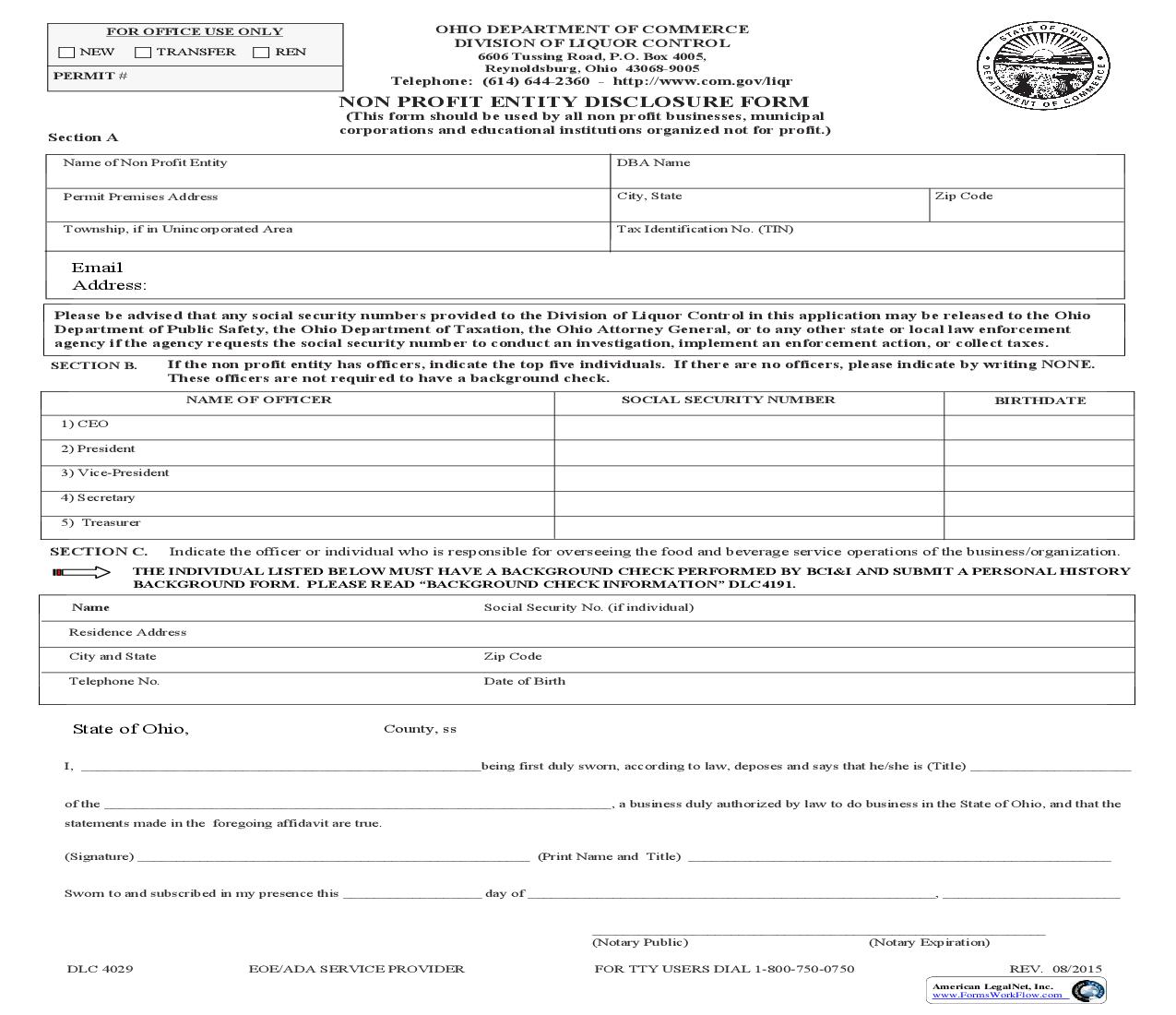
Department Of Commerce
Division Of Liquor Control


Last updated: 3/30/2016
Non Profit Entity Disclosure Form {DLC 4029}
Start Your Free Trial $ 13.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
DLC 4029 -- Non Profit Entity Disclosure Form www.FormsWorkFlow.com
Related forms
-

Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/ -
Ohio/Statewide/Department Of Commerce/Division Of Liquor Control/
Form Preview
Our Products