

Last updated: 4/13/2017
Notice Of Appeal {IC-12}
Start Your Free Trial $ 13.99What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
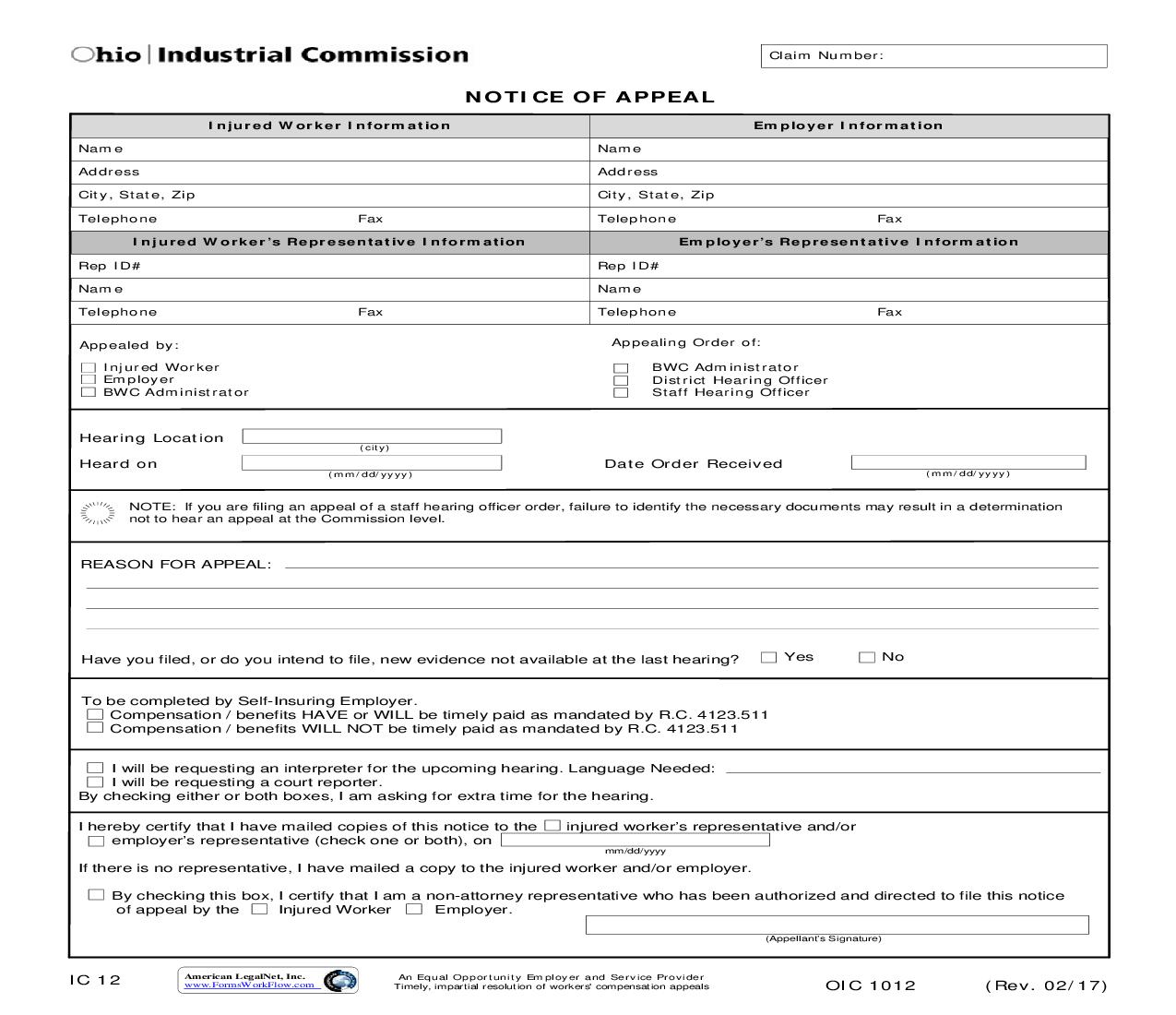
Claim Number: NOTICE OF APPEAL Injured Worker Information Name Address City, State, Zip Telephone Fax Name Address City, State, Zip Telephone Fax Employer's Representative Information Rep ID# Name Fax Telephone Appealing Order of: BWC Administrator District Hearing Officer Staff Hearing Officer Fax Employer Information Injured Worker's Representative Information Rep ID# Name Telephone Appealed by: Injured Worker Employer BWC Administrator Hearing Location Heard on (city) (mm/dd/yyyy) Date Order Received (mm/dd/yyyy) NOTE: If you are filing an appeal of a staff hearing officer order, failure to identify the necessary documents may result in a determination not to hear an appeal at the Commission level. REASON FOR APPEAL: Have you filed, or do you intend to file, new evidence not available at the last hearing? Yes No To be completed by Self-Insuring Employer. Compensation / benefits HAVE or WILL be timely paid as mandated by R.C. 4123.511 Compensation / benefits WILL NOT be timely paid as mandated by R.C. 4123.511 I will be requesting an interpreter for the upcoming hearing. Language Needed: I will be requesting a court reporter. By checking either or both boxes, I am asking for extra time for the hearing. I hereby certify that I have mailed copies of this notice to the employer's representative (check one or both), on injured worker's representative and/or mm/dd/yyyy If there is no representative, I have mailed a copy to the injured worker and/or employer. By checking this box, I certify that I am a non-attorney representative who has been authorized and directed to file this notice of appeal by the Injured Worker Employer. (Appellant's Signature) IC 12 American LegalNet, Inc. www.FormsWorkFlow.com An Equal Opportunity Employer and Service Provider Timely, impartial resolution of workers' compensation appeals OIC 1012 (Rev. 02/17)
Related forms
-

Ohio/Workers Comp/Industrial Commission/ -
Ohio/Workers Comp/Industrial Commission/ -
Ohio/Workers Comp/Industrial Commission/ -
Ohio/Workers Comp/Industrial Commission/ -
Ohio/Workers Comp/Industrial Commission/ -
Ohio/Workers Comp/Industrial Commission/ -
Ohio/Workers Comp/Industrial Commission/ -
Ohio/Workers Comp/Industrial Commission/ -
Ohio/Workers Comp/Industrial Commission/ -
Ohio/Workers Comp/Industrial Commission/ -
Ohio/Workers Comp/Industrial Commission/ -
Ohio/Workers Comp/Industrial Commission/ -
Ohio/7 Workers Comp/Industrial Commission/ -
Ohio/7 Workers Comp/Industrial Commission/ -
Ohio/Workers Comp/Industrial Commission/ -
Ohio/Workers Comp/Industrial Commission/ -
Ohio/Workers Comp/Industrial Commission/