

Last updated: 10/14/2022
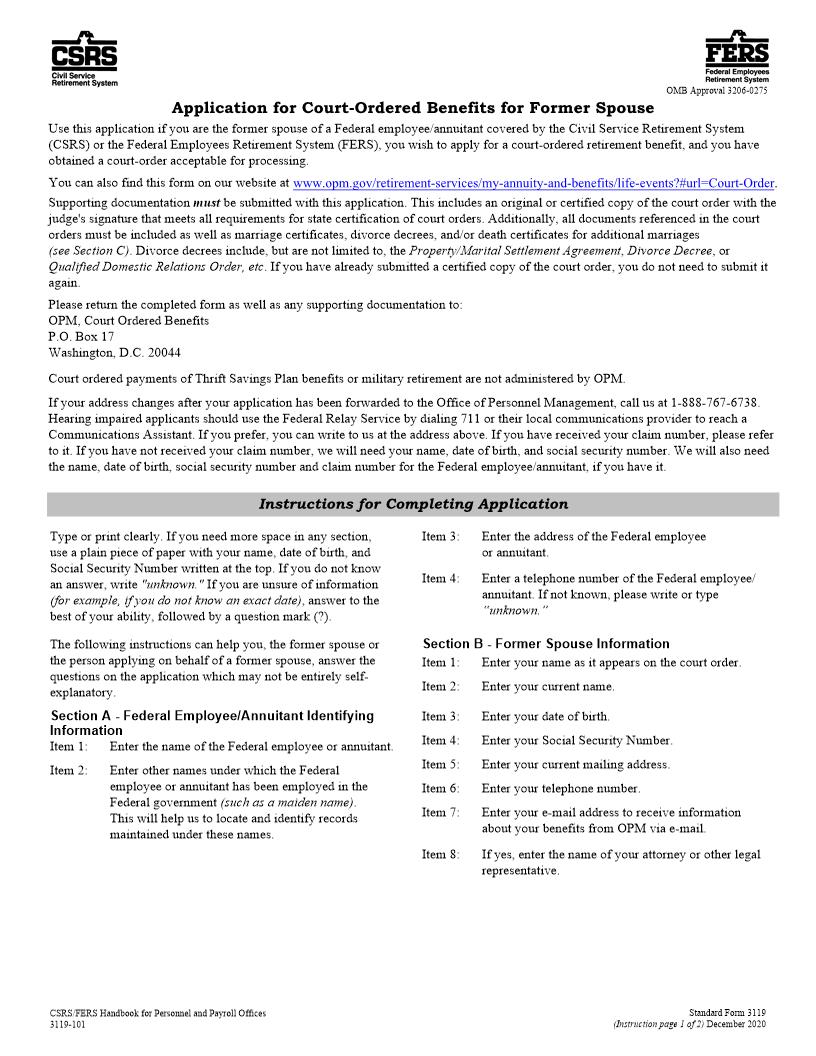
Application For Court-Ordered Benefits For Former Spouse {SF 3119}
Start Your Free Trial $ 18.00What you get:
- Instant access to fillable Microsoft Word or PDF forms.
- Minimize the risk of using outdated forms and eliminate rejected fillings.
- Largest forms database in the USA with more than 80,000 federal, state and agency forms.
- Download, edit, auto-fill multiple forms at once in MS Word using our Forms Workflow Ribbon

- Trusted by 1,000s of Attorneys and Legal Professionals
Description
Certification of Insured Employee's Retired Status Federal Employees Group Life Insurance Federal Employees' Group Life Insurance (FEGLI) Program 2. 5. 7. Date of birth (mm/dd/yyyy) Plan or system under which retired Annuity commencing date (mm/dd/yyyy) 3. 6. 8. Important: Read instructions on the Back of Part 3 before completing this form. A. Agency Report of Insurance Coverage 1. 4. Name of retired employee (last, first, middle) Mailing address (including ZIP code) Social Security number Retirement claim number (if any) Did employee retire on an immediate annuity? Yes 9. Did employee have Basic life insurance for the 5 years immediately before the annuity commencing date or full periods available? Yes If %22Yes%22 check appropriate box No 10. Did employee have Option A -- Standard for the 5 years immediately before the annuity commencing date or full periods available? 75% Reduction No Reduction 50% Reduction Yes 11A. How many multiples of Option B is the employee eligible to carry into retirement? 11B. How many multiples of Option B does the employee want to carry into retirement? ______ No Reduction ______ (number of multiples) ______ (number of multiples) (check one) ______ Full Reduction 12A. How many multiples of Option C is the employee eligible to carry into retirement? 12B. How many multiples of Option C does the employee want to carry into retirement? ______ No Reduction ______ (number of multiples) ______ (number of multiples) (check one) ______ Full Reduction 13. 14. I certify that I obtained the above information, except for periods of unverified service alleged by the retired employee, from official records and it is correct. Name and mailing address of agency (include ZIP code) 15. Signature of authorized agency official 16. Typed name of authorized agency official 17. Date (mm/dd/yyyy) 18. Telephone number (with area code) No B. Certification of the Office of Personnel Management, Boyers, PA 16017 1. Individual named above has Basic life insurance as a retired employee under the Federal Employees' Group Life Insurance Program. Individual named above does not have Basic life insurance as a retired employee because: Not enrolled in Basic for the 5 years immediately before the annuity commencing date or full periods available. Not retired on an immediate annuity. Other (please explain) Option C: 3. OPM Use Only 2. Check the box(es) that apply in line A below if the retired employee has Option A, Option B, or Option C. If you check Option B or Option C, enter the number of multiples. If the individual does not have Option A, Option B, or Option C, check the reason in line B1, B2, B3, or B4. A. Individual named above has this type of Optional insurance as a retired employee under the Federal Employees' Group Life Insurance Program. Option A Option B: Number of Full Reduction multiples __________ Number of No Reduction multiples __________ Number of Full Reduction multiples __________ Number of No Reduction multiples __________ B. Individual named above does not have this type of Optional insurance as a retired employee because: B1. Did not elect this type of Optional insurance as an employee. 4. Signature of authorized OPM official B2. Not eligible for Basic. A B C A B C 5. Typed name of authorized OPM official 6. Date (mm/dd/yyyy) B3. Not enrolled for the 5 years immediately before the annuity commencing date or full period available. B4. Cancelled this type of Optional insurance. A B C A B C C. Agency Report of Termination of Retired Status 1. Reason for termination Death Termination of annuity Other (please explain) 2. Insurance coverage at time of termination Basic: Option A Option B: Number of Full Reduction multiples __________ Number of No Reduction multiples __________ Option C: Number of Full Reduction multiples __________ Number of No Reduction multiples __________ 3. If reason for termination is death, give name and address of next of kin, executor of estate or other contact. 4. Signature of authorized agency official 75% Reduction 50% Reduction No Reduction 5. Typed name of authorized agency official 6. Date annuity terminated (mm/dd/yyyy) 7. Date (mm/dd/yyyy) 8. Telephone number (with area code) U.S. Office of Personnel Management FEGLI Handbook Part 1 - Original 2820-104 Previous editions are not usable. SF 2820 Revised July 2000 American LegalNet, Inc. www.FormsWorkFlow.com Federal Employees Group Life Insurance Certification of Insured Employee's Retired Status Federal Employees' Group Life Insurance (FEGLI) Program 2. 5. 7. Date of birth (mm/dd/yyyy) Plan or system under which retired Annuity commencing date (mm/dd/yyyy) 3. 6. 8. Important: Read instructions on the Back of Part 3 before completing this form. A. Agency Report of Insurance Coverage 1. 4. Name of retired employee (last, first, middle) Mailing address (including ZIP code) Social Security number Retirement claim number (if any) Did employee retire on an immediate annuity? Yes 9. Did employee have Basic life insurance for the 5 years immediately before the annuity commencing date or full periods available? Yes If %22Yes%22 check appropriate box No 10. Did employee have Option A -- Standard for the 5 years immediately before the annuity commencing date or full periods available? 75% Reduction No Reduction 50% Reduction Yes 11A. How many multiples of Option B is the employee eligible to carry into retirement? 11B. How many multiples of Option B does the employee want to carry into retirement? ______ No Reduction ______ (number of multiples) ______ (number of multiples) (check one) ______ Full Reduction 12A. How many multiples of Option C is the employee eligible to carry into retirement? 12B. How many multiples of Option C does the employee want to carry into retirement? ______ No Reduction ______ (number of multiples) ______ (number of multiples) (check one) ______ Full Reduction 13. 14. I certify that I obtained the above information, except for periods of unverified service alleged by the retired employee, from official records and it is correct. Name and mailing address of agency (include ZIP code) 15. Signature of authorized agency official 16. Typed name of authorized agency official 17. Date (mm/dd/yyyy) 18. Telephone number (with area code) No B. Certification of the Office of Personnel Management, Boyers, PA 16017 1. Individual named above has Basic life insurance as a retired employee under the Federal Employees' Group Life Insurance Program. Individual named above does not have Basic li
Related forms
-

Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/ -
Official Federal Forms/US Office Of Personnel Management/Standard/